Committee on Trauma
Formation of the Committee on Fractures
The ACS Board of Regents forms the Committee on Fractures and appoints Charles L. Scudder, MD, FACS, as its first chair. Scudder is seen as an authority on fracture management after his 1900 magnum opus, the Treatment of Fractures.
Over time, the scope of the committee would expand to include other forms of traumatic injury, adding 'and Other Traumas' to the name. It would be officially renamed the Committee on Trauma in 1949.

Committee on Trauma
Dr. Charles Scudder Delivers the First Oration on Fractures
Charles L. Scudder, MD, FACS, delivers the first Oration on Fractures at Clinical Congress. Its name would be changed to the Oration on Trauma in 1952 and, finally, to the Scudder Oration on Trauma in 1963. To be nominated and selected to give the oration remains one of the greatest honors in the field of trauma surgery.

EMS and Systems
Subcommittee Formed to Emphasize the Importance of Immediate Care
The Subcommittee on Ambulance Equipment in the Emergency Treatment of Fractures is created and quickly renamed in 1934 to the Subcommittee on the Transportation of Fractures, later replacing the word 'fractures' with 'injured.' Today’s emphasis on the importance of the trauma continuum of care that begins when and where injury occurs heralds from these initial committees, and is now promoted by the EMS Committee as we know it today.

Committee on Trauma
Fred Bancroft, MD, FACS, Becomes Chair of the Committee on Fractures
Dr. Scudder retires as the original Committee on Fractures chair and is replaced by Fred Bancroft, MD, FACS. Dr. Bancroft helps improve the care of fractures by expanding the committee with surgeons who bring unique perspectives and areas of expertise. He continues Dr. Scudder’s initial focus on use of the sectional committees to expand knowledge and improvements in care around the country.
EMS and Systems
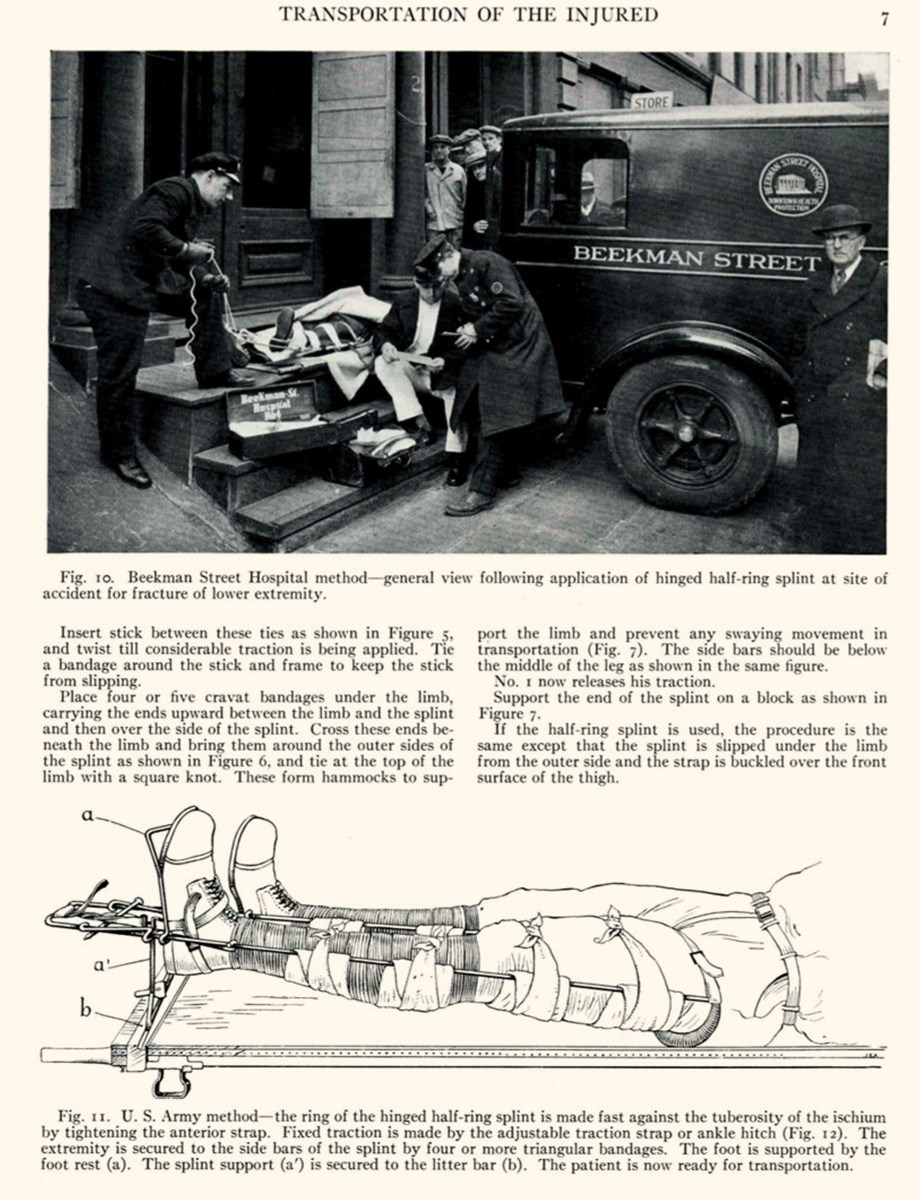
"Transportation of the Injured" Is Published
Dr. Robert H. Kennedy, MD, FACS, publishes the landmark article "Transportation of the Injured," discussing transportation considerations and splinting techniques. The Subcommittee on the Transportation of Fractures follows in 1936. It recommends basic equipment on ambulances and training for responders, beginning the transition of the ambulance attendant from a transporter to a caregiver.
Quality
Robert H. Kennedy, MD, FACS, Becomes Chair of the Committee on Fractures and Other Trauma
ACS merges the Committee on Fractures with the Board on Industrial Medicine and Traumatic Surgery to form the Committee on Fractures and Other Trauma. Robert H. Kennedy, MD, FACS, is appointed chair.
At 13 years, Dr. Kennedy remains the committee's longest serving chair, and is identified in print as "Mr. Trauma U.S.A.," "Father of Trauma Care," or the "King of Trauma" in recognition of his distinguished career helping improve the prehospital and emergency room care of trauma patients.

Committee on Trauma
Third Edition of Fracture Treatment Manual Published
The third Edition of Principles and Outline of Fracture Treatment manual is published, and nearly 45,000 copies are distributed at the request of the armed forces during World War II.
Committee on Trauma
U.S. Advances Trauma Care in WWII
The U.S. enters World War II, during which 407,316 American soldiers are killed and 670,846 wounded. Correspondence between military medical leaders and the Committee on Fractures advances the principles of blood transfusions. This time period also marks the introduction of albumin, phased wound management, the use of sulfonamides (1935), penicillin (1941), and debridement for wound care and fracture splinting practices. Survival rate for the wounded: 50 percent.

Committee on Trauma
U.S. Advances Trauma Care During the Korean War
The U.S. enters the Korean War, during which over 33,000 American soldiers are killed, and 103,284 are wounded. We see advances in helicopter transport and the introduction of forward surgical units (MASH). Army vascular surgeons try to repair major blood vessels rather than perform ligations.
Committee on Trauma
R. Arnold Griswold, MD, FACS, Becomes COT Chair
Dr. Griswold becomes chair of the COT. In his tenure, which lasts until 1957, he oversees the publication of the fifth edition of the Principles and Outline of Fracture Treatment and the publication of the first edition of the Early Care of Acute Soft Tissue Injuries. He begins the long quest to require automobile manufacturers to put more emphasis on occupant safety in automobile design. These requirements would not be imposed by the Department of Transportation for another ten years.
Injury Prevention
Organized Injury Prevention Begins with Concern Over Motor Vehicle Crash Injuries
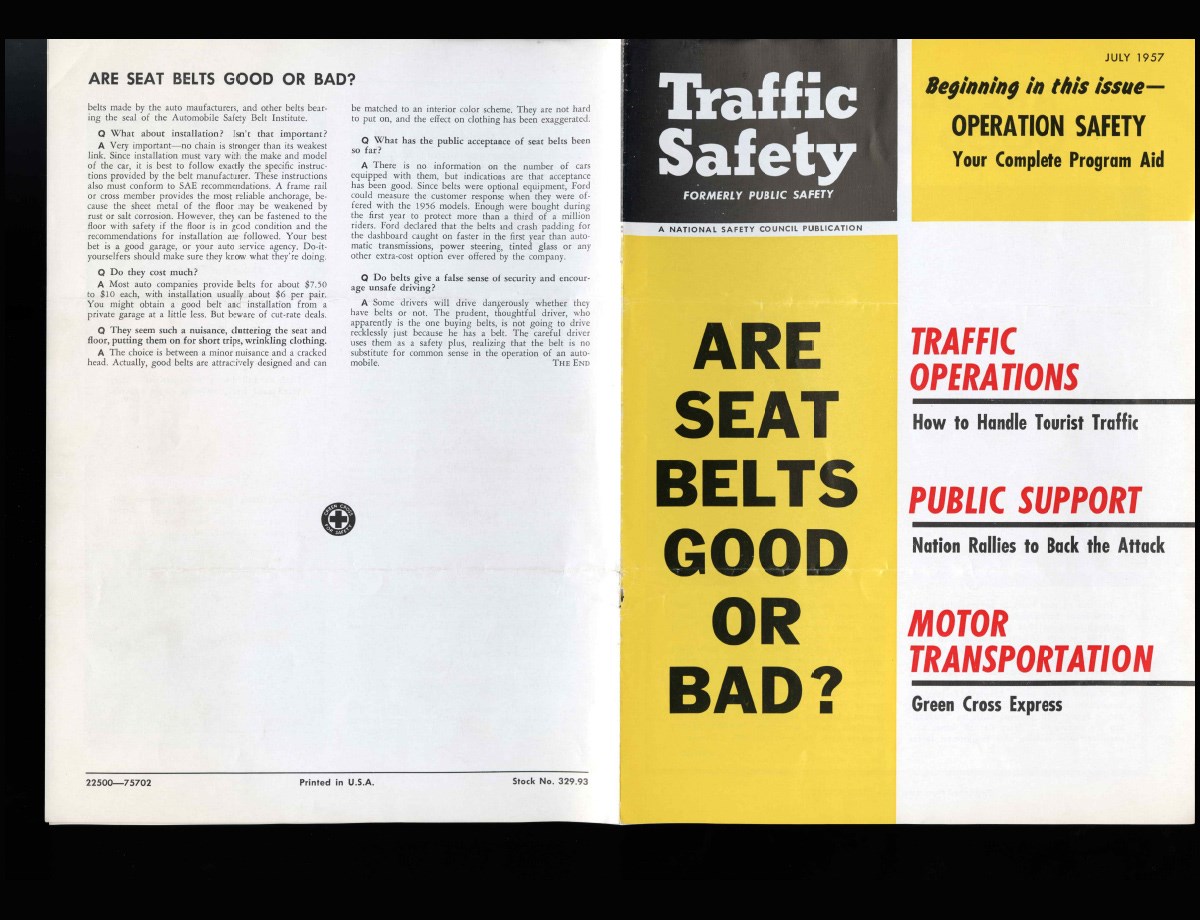
The first COT subcommittee on Traffic Injury Prevention is appointed. The following year, COT Chair Dr. Griswold testifies before Congress to advocate for increased auto safety and the mandatory use of seatbelts. The COT then partners with the American Association for the Surgery of Trauma and the National Safety Council to form the Joint Action Program, which continues these efforts along with a public education campaign implemented by the regional COT. Additionally, the COT takes on the "Big Three" auto manufacturers to promote car safety standards.
Committee on Trauma
Preston A. (Pep) Wade, MD, FACS, Becomes COT Chair
Dr. Wade serves in this role until 1959 when he is named to the ACS Board of Regents. Previously serving as Chair of the Subcommittee on Regional Committees, and authoring the first guide for regional committees, Dr. Wade also is credited with changing the name of the Oration on Trauma to the Scudder Oration on Trauma in 1963.

Committee on Trauma
Harrison L. McLaughlin, MD, FACS, Becomes COT Chair
Dr. McLaughlin serves from 1959 until 1964, and is integral in helping to secure funding to establish the Committee on Trauma Field Program, which directly addresses the need to improve emergency departments and the transportation of the injured.

Quality
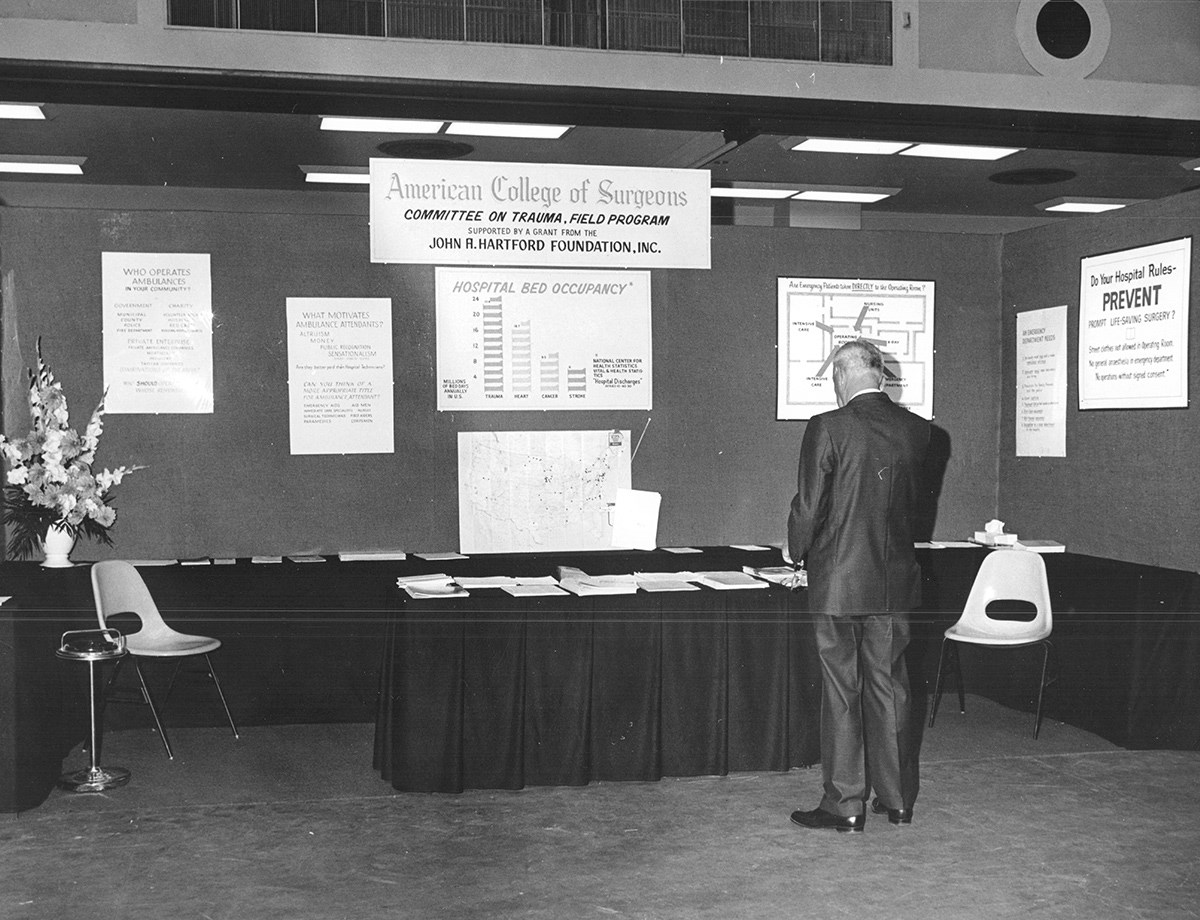
The Committee on Trauma Field Program Is Established
The Committee on Trauma Field Program is established, funded by grants from the John A. Hartford Foundation. Dr. Kennedy is appointed as Director and develops standards for hospital emergency departments and ambulance services. He publishes Model of a Hospital Emergency Department and Guide to Organization and Management of Hospital Emergency Departments. A scale model was produced to illustrate the optimal layout of an emergency department.

Committee on Trauma
Oscar P. Hampton, Jr., MD, FACS, Becomes COT Chair
Dr. Hampton serves as COT Chair from 1964–1968. In this role, he continues the efforts of the Committee on Trauma Field Program to contribute to prehospital and emergency care, and develops a set of Standards for Emergency Ambulance Service in 1967. He would later join the ACS in a staff position and serve as Assistant Director of the ACS and Consultant in Trauma, COT Secretary.

Injury Prevention
National Traffic and Motor Vehicle Safety Act Passed
The National Traffic and Motor Vehicle Safety Act of 1966 mandates the installation of seatbelts and establishes the U.S. Department of Transportation, comprising several travel safety administrations—including what would ultimately become the National Highway Traffic Safety Administration. This Act and subsequent others are passed in large part due to the ardent advocacy of the COT.
EMS and Systems
Accidental Death and Disability: The Neglected Disease of Modern Society Is Published, Starting a “7 Years’ War”
This white paper signifies a seminal moment in the development of emergency medical systems (EMS) and trauma care. Published by the National Academy of Sciences’ National Resource Council, the report underscores the fact that traumatic injury should be considered a major public health problem. The COT continues to escalate its efforts to promote safety measures in automobiles and enhanced training and standards for emergency medical services providers, in what J.D. Farrington, MD, FACS, called the COT’s “7 Years’ War.”

EMS and Systems
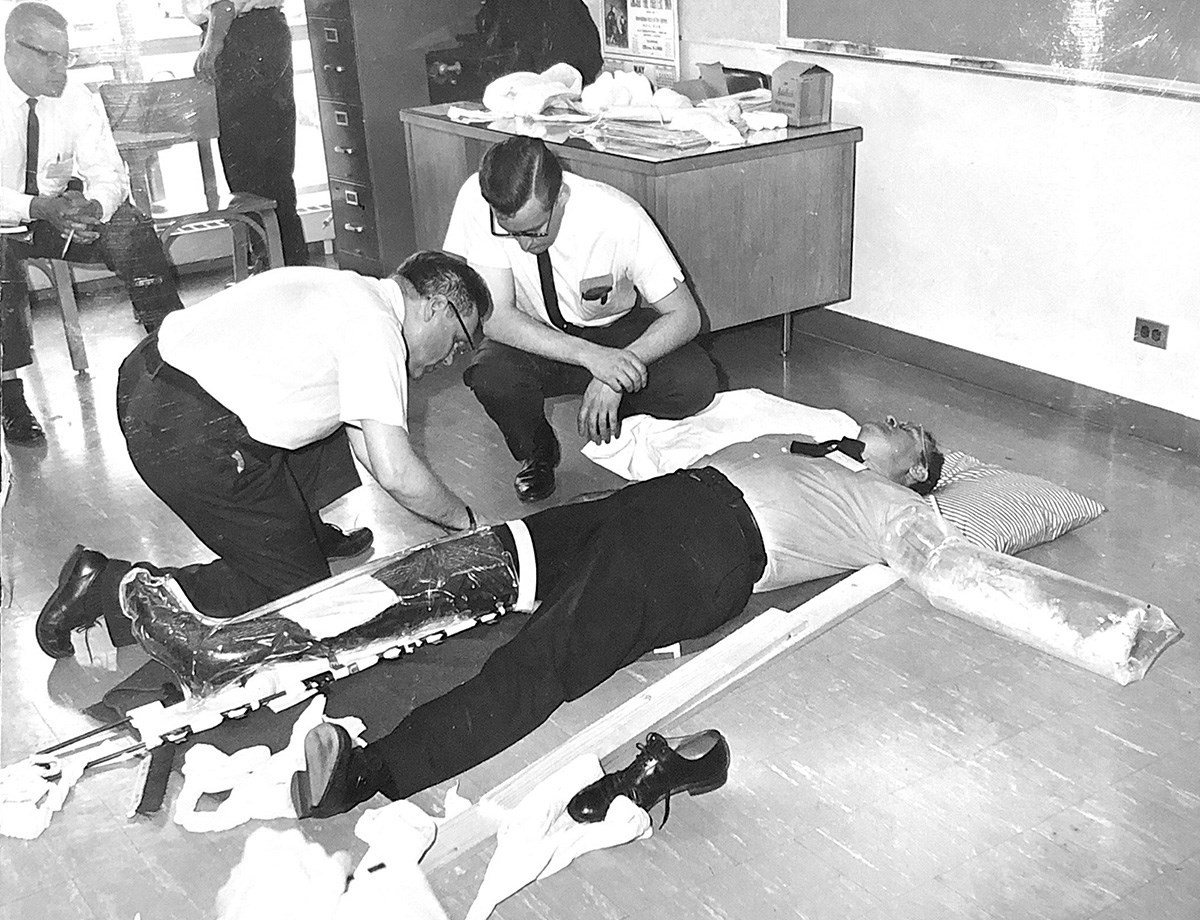
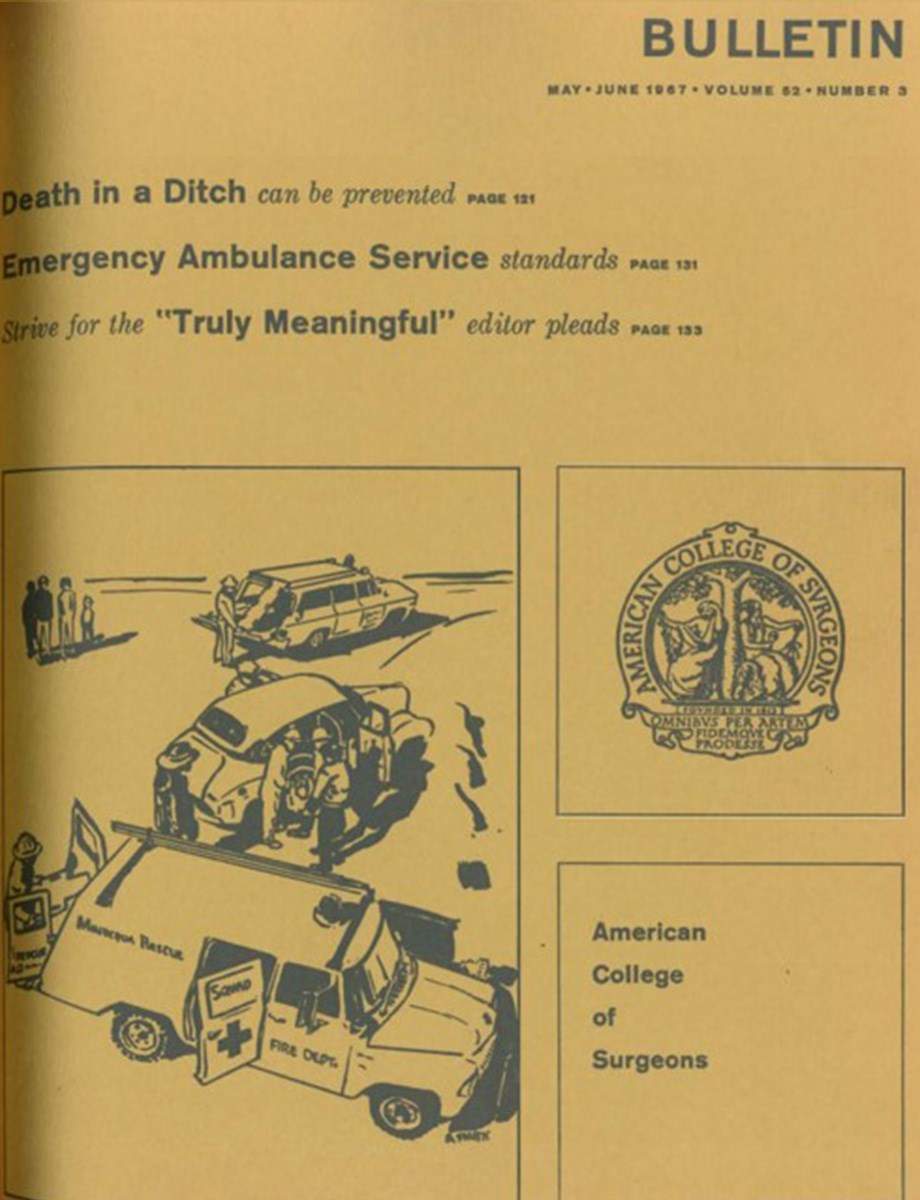
“Death in a Ditch” Published in the ACS Bulletin
Written by Joseph D. Farrington, MD, FACS, Chair, Subcommittee on Transportation of the Injured (1965-1974), this article describes before-and-after scenarios of injured people destined to live or die based on how they’re treated at the scene. In addition, the publication highlights, on a national level, the need for education of field responders and heralds major changes in the provision of initial care following motor vehicle crashes prior to transportation, including the first ambulance equipment list.

Committee on Trauma
Curtis P. Artz, MD, FACS, Becomes COT Chair
Serving as COT chair from 1968–1974, Dr. Artz develops guidelines for the categorization of hospital emergency capabilities, and publishes Early Care of the Injured Patient in 1972—the first publication designed as a compilation of both the fracture manual and soft tissue manual. The regional sections are restructured to match regions defined by the U.S. Department of Health, Education, and Welfare.
Committee on Trauma
Regional COTs Expand Beyond the U.S. and Canada
Global expansion starts with Mexico (1968), Panama (1972), and Colombia (1983). This would lead to the formation of Region 14 (Latin America) in 1987, and by 2011, the expansion would include Region 15 (Europe and parts of Africa), Region 16 (Australasia), and Region 17 (Middle East and North Africa).
Quality
First Trauma Registry Is Catalyst for Data-Driven Quality Improvement
David. R. Boyd, MD, FACS, and colleagues describe the first hospital trauma registry developed to enable research and patient monitoring. This contributes later to the 1982 COT Ad Hoc Task Force on Injury Severity Scoring led by Charles F. Frey, MD, FACS. He proposes that the ACS develop a way for hospitals to submit data for analysis. This subsequently leads to the "Major Trauma Outcomes Study," developed by Howard R. Champion, MD, FACS, which collects data from trauma centers across the U.S. from 1982–1989, establishing national norms to provide predicted risk of mortality that can be used to identify opportunities for quality improvement.
Committee on Trauma
Robert W. Gillespie, MD, FACS, Becomes COT Chair
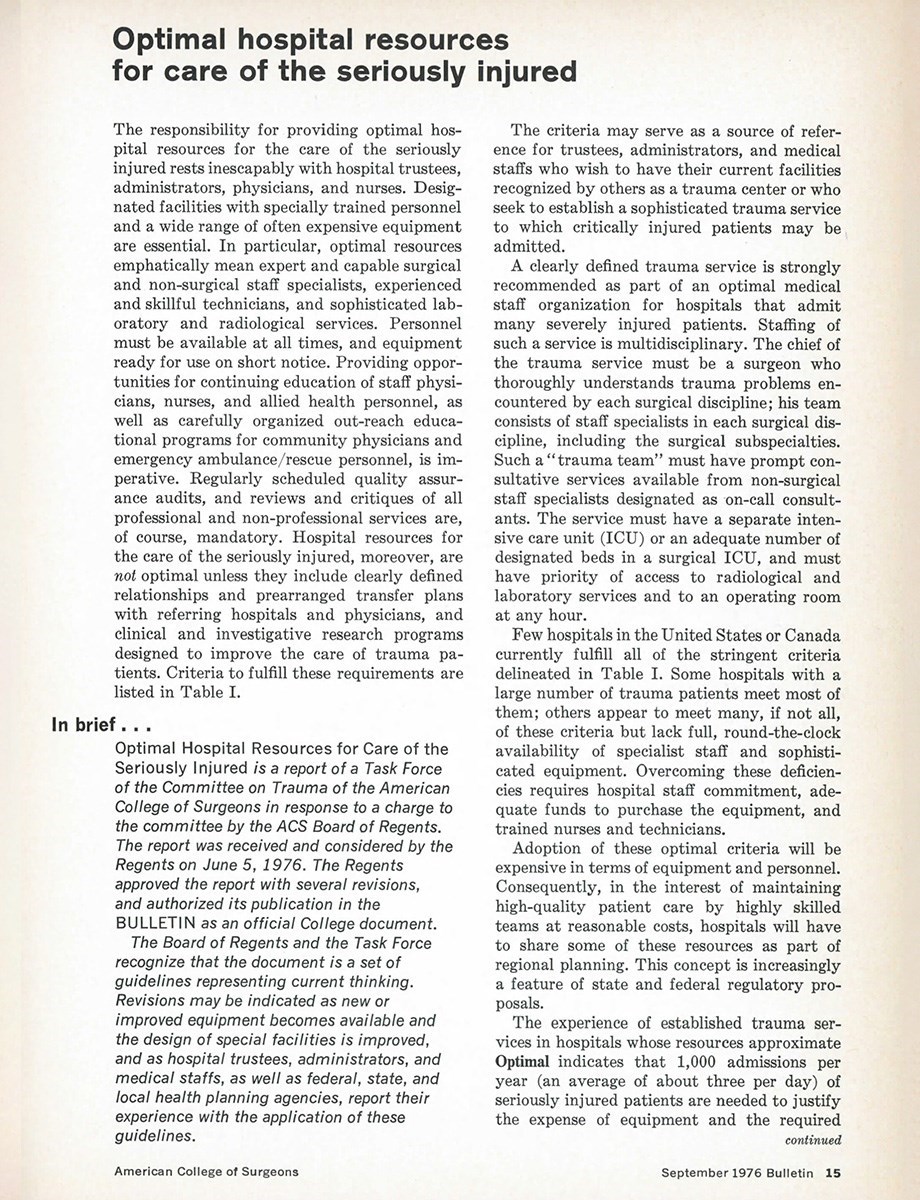
From 1974–1978, Dr. Gillespie plays a key role in developing the Advanced Burn Life Support Provider Course and the Pre-Hospital Burn Life Support Course. During his tenure as Chair, the "Optimal Hospital Resources for Care of the Seriously Injured" is published in the September 1976 issue of the ACS Bulletin, setting in motion subsequent efforts towards a verification process for trauma centers.
Quality
The COT Publishes “Optimal Hospital Resources for Care of the Seriously Injured”
This is the first edition of "Optimal Hospital Resources for Care of the Seriously Injured," now known as Resources for Optimal Care of the Injured Patient. This change from "optimal hospital resources" to "optimal care, given available resources" reflects an abiding principle: the needs of injured patients must be addressed both at the point of injury and wherever they receive care.
Committee on Trauma
C. Thomas "Tommy" Thompson, MD, FACS, Becomes COT Chair
During his tenure from 1978–1982, Dr. Thompson presides over the initial phases of developing the Capital Program, established following the assassination attempt on President Reagan to identify trauma providers around the country for emergency care for high-profile government members. Dr. Thompson also helps lead the national expansion of the Advanced Trauma Life Support® (ATLS®) program, establishes the Military COT Region 13, and helps introduce an early concept for trauma center verification.

Committee on Trauma
First Resident Trauma Papers Competition
First known as the Regional Resident Award Program, it is conceived by Charles F. Frey, MD, FACS, and organized by Henry C. Cleveland, MD, FACS, as a national competition. John A. Weigelt, MD, FACS, is the first winner. Today, the competition is open to all general surgery residents, surgical specialty residents, and trauma fellows. Original research on any aspect of trauma care can be submitted. Finalists are selected from COT regions around the world, and invited to the COT Annual Meeting where they present their papers.

Education
First COT ATLS Course Held in Lincoln, Nebraska
After a 1976 plane crash kills his wife and injures his children and himself, James K. Styner, MD, FACS, develops the Advanced Trauma Life Support® (ATLS®) course in 1978 to train providers in the early management of the injured patient. In 1980, ATLS would become the flagship course of the Committee on Trauma. Today, more than one million providers have been trained in ATLS in 84 countries worldwide.

Committee on Trauma
COT Establishes a Formal Military Region
The ACS announces that a formal military region (Region 13) will be established within the COT. Region 13 includes a Region Chief and chairs from each of the U.S. military services (Army, Navy, Air Force), the Veterans Administration, and the Canadian Forces. The inaugural chair is Norman M. Rich, MD, FACS, DMCC, MC, department of surgery, Uniformed Services University of the Health Sciences (USUHS), Bethesda, MD.

Committee on Trauma
Donald D. Trunkey, MD, FACS, Becomes COT Chair
Dr. Trunkey ushers in the modern era of the COT. As chair from 1982–1986, he develops a position statement outlining the need for a regionalized system of care and the need for trauma center review and designation. He also issues a request to the Board of Regents to permit the development of standards by the COT for accreditation of trauma centers—and to allow the COT to help implement those standards. In 1983, Dr. Trunkey would charge the COT to develop disaster plans for hospitals, leading to the endorsement of the National Disaster Medical System (NDMS), a public-private partnership between the federal government and private health care institutions that provides medical evacuation and definitive care following disasters.

EMS and Systems
Norman E. McSwain, Jr., MD, FACS, Oversees Development of the PHTLS Course
Dr. McSwain chairs the Subcommittee on Emergency Services – Prehospital from 1981–1986. A founding member of the National Association of Emergency Medical Technicians (NAEMT), he leads the development of the early Prehospital Trauma Life Support (PHTLS) Course, based on the COT’s ATLS Course for physicians. Because of his vision, the NAEMT’s PHTLS Course ultimately becomes the "gold standard" for prehospital trauma education worldwide, and there’s always been a close, symbiotic relationship between the ACS COT and NAEMT, ATLS, and PHTLS.
Injury Prevention
COT Forms the Ad Hoc Trauma Prevention Committee
Early injury prevention by the COT largely focused on motor vehicle crashes and firearm injury, but its continual evolution leads to the creation of the Ad Hoc Trauma Prevention Committee in 1985 under the tenure of Donald Trunkey, MD, FACS. In 1998, this Ad Hoc Committee would be renamed to the Injury Prevention and Control Committee (IPCC), recognizing injury as a public health issue and positioning the COT as national leaders in injury prevention.
Quality
Ad Hoc Committee on Quality Assurance Heralds New Approach to Quality Care
This committee is appointed by Donald D. Trunkey, MD, FACS, with Frank L. Mitchell, Jr., MD, FACS, as the first chair. It would later be renamed to the COT Quality Improvement Subcommittee, and then the Performance Improvement and Patient Safety (PIPS) Committee. This committee in all its iterations works to combine measurable data and education of best practices to advance the quality of patient care.

Quality
The ACS Board of Regents Approves COT Recommendations for a Verification Program
After several long years of advocacy for a verification program, implementation begins for a true trauma verification program under the direction of the COT, expanding the standardization of trauma care.
Committee on Trauma
Erwin R. Thal, MD, FACS, Becomes COT Chair
Chair from 1986–1990, Dr. Thal continues the work of Drs. Thompson and Trunkey to establish a Trauma Verification Program and to revise and strengthen the Hospital and Prehospital Resources for Optimal Care of the Injured Patient and Appendices A through J manual. Other accomplishments include Board of Regents’ approval for promulgation of the ATLS course outside of the COT organizational structure, with the first course held in London, UK, in November 1988.

EMS and Systems
First Guidelines for Field Triage of Injured Patients Published
These initial guidelines establish local emergency medical service triage protocols. They were revised in 1990, 1993, and 1999. In 2005, the COT works with the National Highway Traffic Safety Administration (NHTSA) and the Centers for Disease Control and Prevention (CDC) to support the evidence-based revision of these guidelines with an expert panel and publishes them in 2006 in Resources for the Optimal Care of the Injured Patient. Subsequent revisions publish in 2009, 2011, and 2022.
Quality
The Verification, Review, and Consultation (VRC) Program Begins
The Verification, Review, and Consultation (VRC) Program of the COT is formally established in 1987, under the leadership of Frank L. Mitchell, Jr., MD, FACS, and enthusiastic support by Erwin R. Thal, MD, FACS, the COT Chair. The program is designed so expert reviewers can evaluate whether a trauma center meets the criteria outlined in Resources for the Optimal Care of the Injured Patient. The first Level I Trauma Center is verified the same year, followed by the first Level II verification in 1988, and the first Pediatric Trauma Center Consultation in 1989.
Quality
The COT Introduces the "Broken Man"
The publication of the Resources for the Optimal Care of the Injured Patient (the "Red Book") introduces the "Broken Man" image—the universally recognized and beloved icon representing the injured patient and representing the focus for all of our efforts. Our Broken Man reminds us why we chose trauma as our calling.
Committee on Trauma
A. Brent Eastman, MD, FACS, Becomes COT Chair
Chair from 1990–1994, Dr. Eastman works to integrate the meetings of the central COT with state chairs and region chiefs. He serves as the first chair of the Ad Hoc Committee on Trauma System Consultation and helps put trauma systems in place on six different continents. Over time, additional accomplishments will include the development of a revised version of the Resources for Optimal Care of the Injured Patient, the Blue Book, and hosting the first International ATLS Meeting at the ACS Clinical Congress in 1993.
Committee on Trauma
John A. Weigelt, MD, DVM, FACS, Becomes COT Chair
Chair from 1994–1998, Dr. Weigelt establishes an Ad Hoc Committee on Rural Trauma to bring more focus to rural trauma care. He also establishes the Working Group for Trauma System Evaluation chaired by Dr. Eastman. The group is charged with developing guidelines to evaluate a trauma system as well as a process for onsite evaluation.

Quality
National Trauma Data Bank® Workgroup Established
A workgroup is established to develop the National Trauma Data Bank® (NTDB) under David B. Hoyt, MD, FACS, Chair of the Subcommittee on the Trauma Registry. J. Wayne Meredith, MD, FACS, MCCM, is appointed as its first lead. The initial data dictionary contains 86 data points and the software for data collection is launched in 1997. The first NTDB annual report is published in 2001, based on 181,000 records, and grows to a milestone number of 1.1 million records in 2004.
Committee on Trauma
David B. Hoyt, MD, FACS, Becomes Chair of the COT
David B. Hoyt, MD, FACS, becomes COT Chair, leading key initiatives like a revision of Resources for Optimal Care of the Injured Patient, expansion of the Trauma Verification Program, global expansion of ATLS, and codification of specialty engagement through the formation of specialty positions and committees.
Under his direction, the COT increases its focus on disaster preparedness and would become a home for disaster management education after the September 11, 2001 attacks. In a new paradigm, Dr. Hoyt becomes the first past chair to then serve as COT Medical Director, and later would go on to become Executive Director of the ACS in 2009.

EMS and Systems
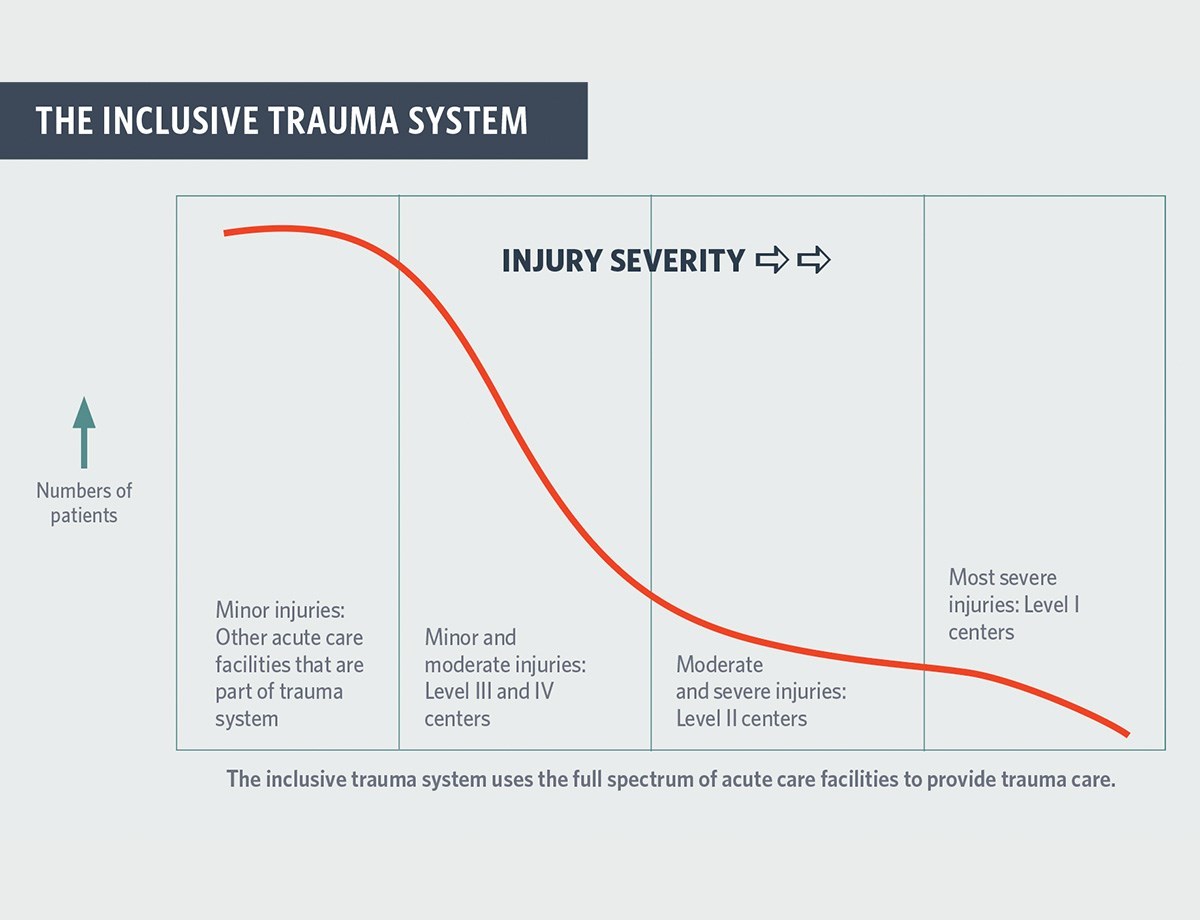
Ad Hoc Committee on Trauma Systems Begins Consultations
The expansion of trauma centers highlights the need for the development of an inclusive trauma system model in which all health care facilities in a region provide care to the extent of their capacity. The Ad Hoc Committee on Trauma System Consultation, chaired by A. Brent Eastman, MD, FACS, formalizes the COT’s commitment to help trauma systems develop and improve through a consultative process. The program's first official consultation visit happens that year in Montana. Though successful, the pilot visit underscores growth areas for the program. "We kind of re-wrote the whole thing based on the lessons learned," Dr. Eastman later says.
Education
ATOM® Course Launches
Lenworth Jacobs, Jr., MD, MPH, FACS, launches his course in Advanced Trauma Operative Management (ATOM®), training surgeons in the operative management of penetrating injury. The ATOM Course is now in its third edition, under the leadership of Jody Kaban, MD, FACS, and has been offered in more than 16 countries


Committee on Trauma
J. Wayne Meredith Becomes Chair of the COT
Wayne Meredith, MD, FACS, becomes COT Chair. During his tenure, he spearheads several important initiatives: reinstituting the Ad Hoc Committee on Disaster and Mass Casualty Management, overseeing further revisions to the Resources for Optimal Care of the Injured Patient, and reorganizing efforts around the National Trauma Data Bank®.
After a change to the Longmire Rules eliminates senior membership status, Dr. Meredith works to increase the number of active members on the central COT and begins intentional efforts to create a more diverse and inclusive environment throughout the COT.

Committee on Trauma
Disaster and Mass Casualty Subcommittee Resurrected
The COT's Disaster and Mass Casualty Subcommittee is resurrected following the September 11, 2001 attacks, with Eric (Rick) Frykberg, MD, FACS, as the Chair. The next year, the COT would publish a statement calling on surgeons to take a leadership role in disaster planning.

Education
Rural Trauma Team Development Course Launched
The Rural Trauma Subcommittee presents the first Rural Trauma Team Development Course in Sisterville, West Virginia. The course emphasizes a multidisciplinary team approach, recognizes the need for minimal equipment requirements, addresses the potential delays and transfer challenges in rural trauma care, and is delivered at a reasonable cost and with substantial flexibility.

Education
Disaster Management and Emergency Preparedness Course Launched
The first Disaster Management and Emergency Preparedness (DMEP) Course is presented in Michigan, and the first DMEP Course manual is published in 2010. Many of the course’s principles were those emphasized by Dr. Robert H. Kennedy 35 years earlier.
Committee on Trauma
John Fildes, MD, FACS, Becomes COT Chair
John Fildes, MD, FACS, becomes chair of the Committee on Trauma. During his tenure, the COT will publish Regional Trauma Systems: Optimal Elements, Integration and Assessment-System Consultation Guide—also known as the White Book—in 2008. In addition, the TQIP program would be formally launched in 2010, and the COT expands delivery of the Disaster Management and Emergency Preparedness Course. Dr. Fildes also oversees the transition to the ninth edition of ATLS and supports the rapid global growth of the COT.

Education
First ASSET Course Held at USUHS
The first Advanced Surgical Skills for Exposure in Trauma (ASSET) Course is taught at Uniformed Services University of the Health Sciences, adding a second Surgical Skills Course (along with ATOM) to the roster of the COT's Ad Hoc Committee on Surgical Skills. Now in its second edition, the course offers a two-day, expanded version called ASSET + (ASSET Plus), which has been developed and fielded through the cooperation of the COT, USUHS, and the Military Health System Strategic Partnership of the American College of Surgeons under the leadership of Mark Bowyer, MD, FACS.

Quality
TQIP Launches
The Trauma Quality Improvement Program (TQIP) launches with Avery Nathens, MD, FACS, as chair. This grew out of a Subcommittee on Trauma Registry Programs project team convened in 2006, charged to pilot and launch a program to provide risk-adjusted outcomes to participating trauma centers. By 2021, there would be more than 875 hospitals enrolled, including Level I, II, III, and Pediatric centers.

Committee on Trauma
Michael F. Rotondo, MD, FACS, Becomes Chair of the COT
Appointed chair of the COT in 2010, Michael F. Rotondo, MD, FACS, oversees the ongoing growth of the ACS core programs and the 2014 revision of the Resources for Optimal Care of the Injured Patient (the "Orange Book"). Most importantly, he leads a military-civilian effort to codify the structure and function of the military’s Joint Trauma System (JTS), resulting in a collaborative book illustrative of the growing partnership between the military and the ACS COT.

Injury Prevention
ACS COT Issues Bold Statement on Firearm Injury Prevention
This statement is driven by the dual tragedies of the 2012 Sandy Hook Elementary School shootings and the Boston Marathon bombing in 2013. The statement includes specific recommendations for injury prevention efforts and promotes evidence-based research on firearm injury. This is the beginning of a major strategic focus on reducing death and disability from firearm injury using the public healthcare model promoted by Ronald M. Stewart, MD, FACS, who works to build bridges between disparate views.


Injury Prevention
First Conference of the Hartford Consensus
A few months after the Sandy Hook shooting, the Joint Committee to Create a National Policy to Enhance Survivability from Intentional Mass Casualty and Active Shooter Events is convened by the ACS with representatives from the medical community, federal agencies, the National Security Council, the U.S. military, and EMS. Over a series of four meetings, the committee jointly develops a series of recommendations that become known as The Hartford Consensus and support early hemorrhage control at the scene, an integrated response by law enforcement and EMS, and public education to support national resilience.

EMS and Systems
New Guidelines Emerge for EMS Providers in External Hemorrhage Control
Eileen M. Bulger, MD, FACS, EMS Committee Chair from 2012–2015, convenes an expert panel to conduct a literature review and make recommendations on external hemorrhage control for EMS providers. The group publishes guidelines that support the use of tourniquets and wound packing with hemostatic agents. The COT subsequently supports efforts to train EMS and law enforcement providers in these vital skills, contributing to the development of the STOP THE BLEED® course.
Quality
Pediatric TQIP and TQIP Collaboratives launch
Pediatric TQIP, led by Michael L. Nance, MD, FACS, FAAP, launches to provide a similar approach to quality improvement for pediatric trauma patients and risk-adjusted benchmarking for pediatric trauma centers. TQIP Collaboratives debuts this same year to provide a self-identified group of trauma centers, typically defined by the state. These collaboratives help identify opportunities for improvement across the group and to facilitate better performance.

Committee on Trauma
Military Health System Strategic Partnership American College of Surgeons (MHSSPACS) Established
Under the leadership of medical director M. Margaret Knudson, MD, FACS, MHSSPACS focuses on educational opportunities, systems-based practices, research endeavors, quality improvement programs, combat readiness, and disaster preparedness. This partnership provides long-term benefits to surgical care in both garrison and combat arenas with readily translatable lessons to civilian surgical practice.


Committee on Trauma
Ronald M. Stewart, MD, FACS, Becomes COT Chair
As COT Chair (2014–2018), Dr. Stewart takes on the challenge of establishing an effective approach to firearm injury prevention. His philosophy is to start with a "common American narrative." That takes a nonpartisan public health approach to build consensus and implement programs that focus on firearm safety for gun owners—and also identifies and treats the root causes of violence.

Committee on Trauma
Coalition for National Trauma Research (CNTR) Is Formed
COT joins AAST, EAST, WTA, and the National Trauma Institute to form the CNTR. Its mission is to enhance trauma research in the U.S. by advocating for sustainable research funding commensurate with the burden of disease, coordinating research efforts across professional organizations that span the continuum of injury care, and strengthening the infrastructure for multicenter investigation.
Committee on Trauma
Future Trauma Leaders (FTL) Program Established
FTL is developed as part of the larger Mentoring for Excellence in Trauma Surgery (METS) program. It engages trauma surgeons in their first 5 years of practice and helps provide an important perspective to the COT leadership on the needs of young surgeons. It also develops a group invested in the COT who can become future leaders in trauma. The inaugural group of 4 FTLs is joined by the Resident and Associate Society and Young Fellows Association liaisons to the COT in the METS program.

EMS and Systems
STOP THE BLEED® Campaign Launches at the White House
The White House event, organized by the National Security Council, puts emphasis on the recommendations of The Hartford Consensus and the bleeding control course. The COT, under license from the Department of Defense, promulgates a full program to provide training in bleeding control and to establish the presence of bleeding control materials in public areas. This successful initiative continues to train people in the steps necessary to control life-threatening bleeding, turning them into initial responders able to save a lives in the face of severe bleeding.

Education
The COT Adds the BEST Course
Developed by Megan Brenner, MD, FACS, the Basic Endovascular Skills for Trauma (BEST) Course focuses on endovascular hemorrhage control using resuscitative endovascular balloon occlusion of the aorta (REBOA).

Committee on Trauma
COT Chair Advances Trauma Systems
As Chair, Dr. Ronald M. Stewart leads the COT in responding to the National Academies of Sciences, Engineering, and Medicine (NASEM) Report on the need for a national trauma system and improved military-civilian integration. He organizes a multidisciplinary conference at the National Institutes of Health to develop strategies to implement the report’s recommendations and makes it COT’s mission to advance this work. He also advances the concept of trauma systems as the framework for disaster response and leads the promulgation of the STOP THE BLEED® program.

Quality
Global Standards Project Conceived
A group led by Maria Fernanda Jimenez, MD, FACS, translates Optimal Resources for the Care of the Injured Patient into Spanish and Portuguese. In addition, the first international trauma center consultation site visit is conducted in Region 14 in Uruguay at the Hospital Maciel in Montevideo. It’s an extension of analyzing each of the U.S. standards, then looking at the country- or region-specific variables that need to be defined in order to tailor the standards to any given region.

Injury Prevention
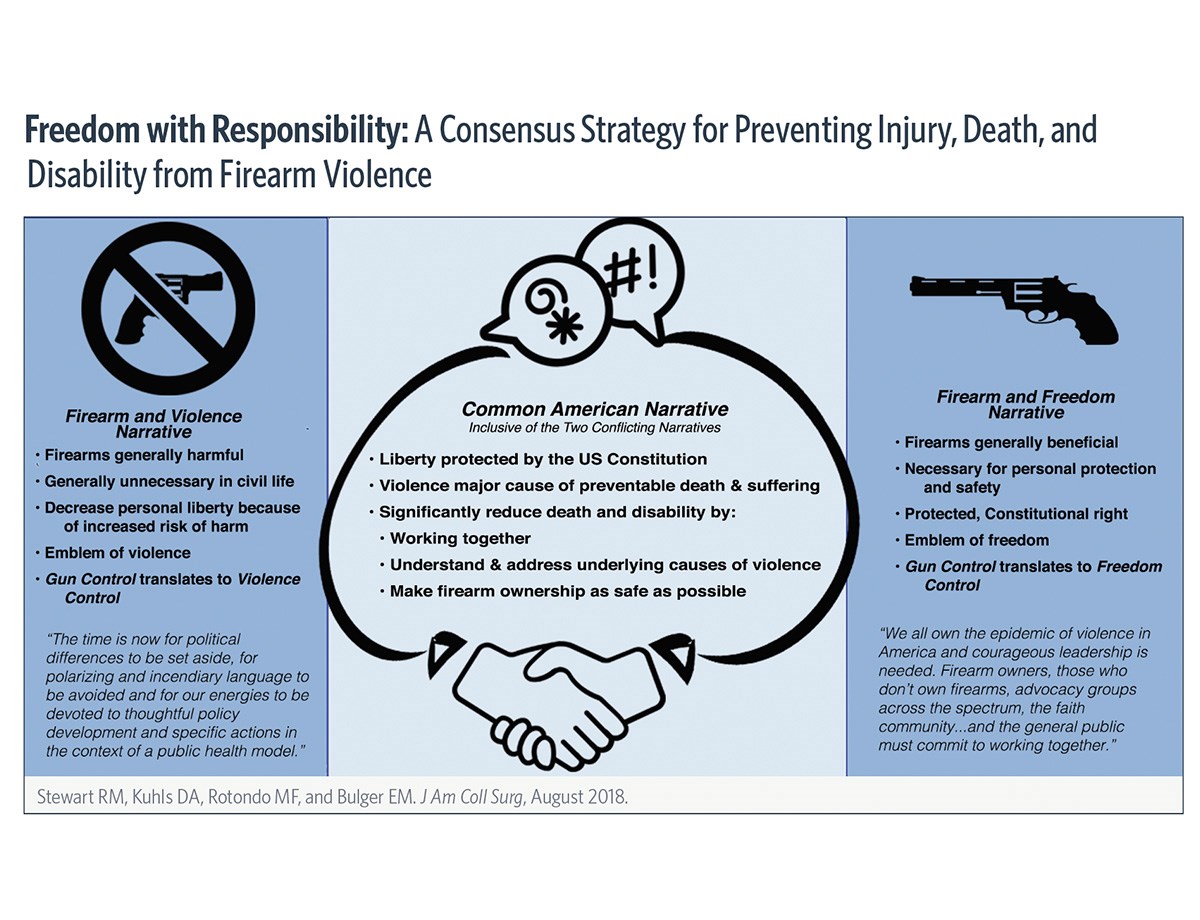
Development of the FAST Work Group
As the Stoneman Douglas High School shooting in Parkland, FL, leaves 17 dead and 17 wounded, the Firearm Strategy Team (FAST) Work Group, led by Dr. Ronald Stewart, develops a consensus strategy on Firearm Injury Prevention. The group publishes its recommendations to reduce firearm-related injury, death, and disability in the U.S.
Committee on Trauma
Eileen M. Bulger, MD, FACS, Becomes COT Chair
Chair from 2018–2022, Dr. Bulger implements a massive strategic planning process, updating the vision and mission statement and reorganizing the activities of the COT. During her tenure, she also renews the COT’s focus on research activities, supports the development of a research infrastructure within TQIP, hosts the CNTR methodology conference to advance trauma research, helps restructure the Coalition for National Trauma Research with the ACS COT as a core member, and wins the National Trauma Research Action Plan Grant for CNTR's efforts.

Committee on Trauma
FTL100 Fundraising Campaign Kicks Off
Under the leadership of Dr. Bulger, the FTL100 and Centennial Campaigns raise more than $1 million. These funds ensure that the COT’s FTL and mentoring programs will be self-sustaining and that the COT can engage in these important mentoring activities well into the future.

Injury Prevention
Medical Summit on Firearm Injury Prevention
The COT leads the historic convening of 44 leading U.S. professional organizations at the 2019 Medical Summit on Firearm Injury Prevention in Chicago, IL— the same year as the mass shooting at a Walmart in El Paso, TX, leaves 23 dead and 23 wounded. Leaders from these organizations discuss developing a public health approach to minimize death and disability related to firearm injuries. The published proceedings provide a roadmap for the implementation of practical interventions.

Injury Prevention
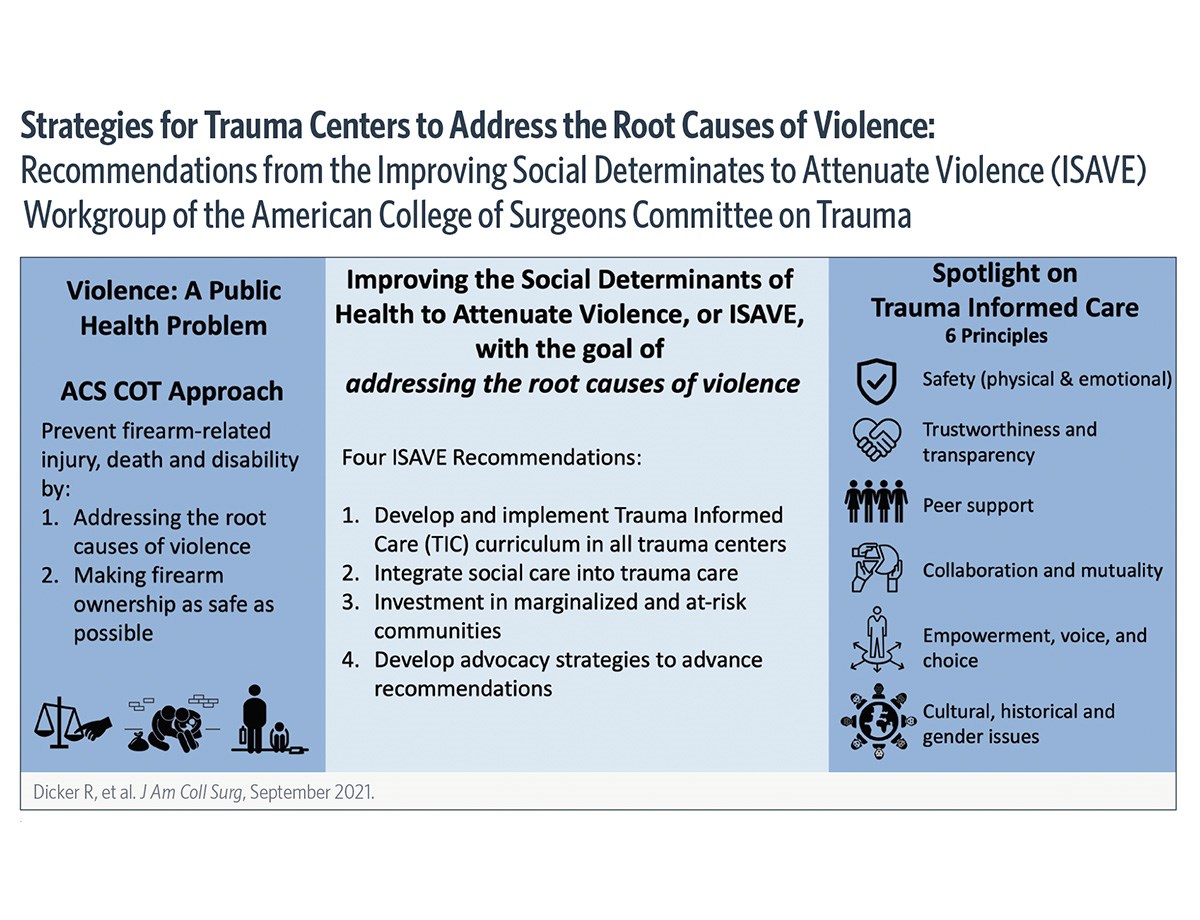
The COT Establishes the ISAVE Work Group
The Improving the Social Determinants to Attenuate Violence (ISAVE) Work Group, led by Rochelle A. Dicker, MD, FACS, is a multidisciplinary group focused on creating a more holistic approach to care for the survivors of violence. The group identifies four primary ISAVE initiatives in their first meeting: (1) develop a trauma-informed care curriculum, (2) invest in at-risk communities, (3) integrate social care into trauma care, and (4) advocacy.
Committee on Trauma
The COT Appoints a Diversity, Equity, and Inclusion (DEI) Work Group
The DEI Advisory Work Group is appointed with Lillian Kao, MD, FACS, as Chair, and conducts a comprehensive survey of COT membership. The group develops a COT Statement on DEI outlining core principles and a multifaceted approach to address areas of opportunity identified in the survey. The broad scope of work ranges from expanding the diversity of candidates for membership or award programs to the reduction of bias in COT educational programs, and beyond.

Education
The COT Adds Dr. Briggs' ADMR Course
The Advanced Disaster and Medical Response (ADMR) Course, offered for many years through Harvard Medical School, is generously donated to the ACS COT Disaster Education portfolio. It will be released as an online course by the COT in 2022.

Injury Prevention
First ACS COT Firearm Injury Prevention Clinical Scholar in Residence
The COT welcomes Arielle Thomas, MD, as the first clinical scholar in this program. This two-year fellowship program provides mentored research experience in injury prevention research and health policy, and is made possible through collaboration between the COT, AFFIRM, AAST, EAST, and the Western Trauma Association (WTA). Brendan T. Campbell, MD, FACS, serves as one of her mentors.

Committee on Trauma
COVID-19 Pandemic
In the age of COVID-19, COT displays dedication, compassion, and flexibility as it works to convert live meetings, courses, site visits, and conferences to remote and virtual endeavors—and to keep the work of the COT moving forward.
EMS and Systems
Creating the Blueprint for a National Trauma and Emergency Preparedness System
COT Advocacy and Systems committees collaborate to create a blueprint for National Trauma and Emergency Preparedness System legislation. This includes support to develop state and regional trauma systems and implement trauma system standards, as well as an interconnected network of Regional Medical Operations Centers (RMOCs) to support the distribution of patients and resources as needed to optimize the response in a region, and allow for coordination at the state and federal levels.
EMS and Systems
COT Offers Guidance During the COVID-19 Pandemic
COT leadership establishes guidance for the formation of Regional Medical Operations Centers (RMOC) to help manage the demands of the pandemic. The goal of the RMOC is to strengthen regional care delivery through enhanced coordination. This model defines and advocates for structural and functional capabilities that enable a region's health care system to "load balance" patient care during a time of crisis.